The operating microscope in dentistry increases the success rates of root canal treatments from 75-85% to over 90-95%, allows you to locate root canals invisible to the naked eye and reduces the amount of healthy tissue removed during each procedure. At Studio Buniato in Corso Francia 30 in Turin, the Leica M525 microscope with magnifications up to 25× is integrated into every phase of the endodontic and microsurgical treatment.
What does the microscope see that the eye does not see?
The human eye has a resolving power of approximately 0.2 mm. Many critical tooth structures — root fractures, accessory canals, perforations, prosthetic margins — are below that threshold. Working without magnification on these structures means operating partly blind, compensating with experience for what is lacking in vision.
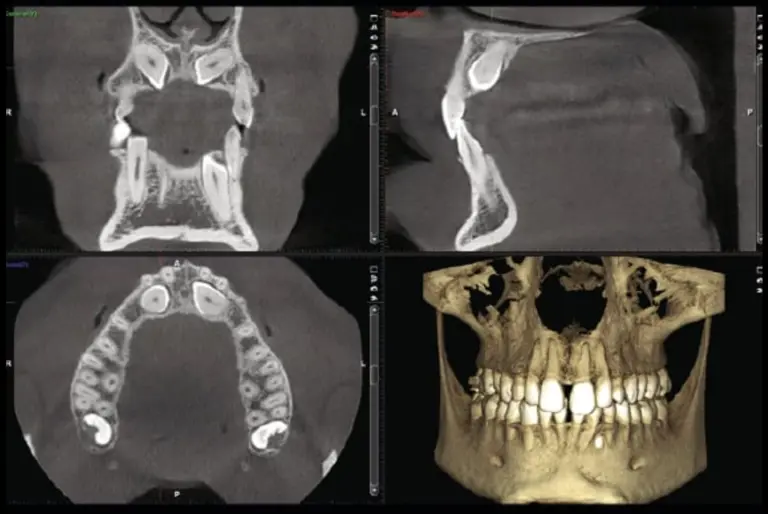
The Leica M525 operating microscope from Studio Buniato offers progressive magnifications from 3× to 25×, with coaxial LED illumination that eliminates shadows inside the root canal. At 16×, channels with a diameter of 0.1 mm are displayed. At 25× vertical fractures are inspected which also escape the CBCT radiography.
The difference between surgical microscopes and common magnifying systems (loupes) is not only quantitative. The loupes offer 2-6× with non-coaxial front light. The microscope offers stable stereoscopic field, constant depth of field, shadow-free illumination and integrated video documentation of every procedure.
Endodontics under the microscope: why numbers matter
The scientific literature is unequivocal. The systematic review by Setzer and colleagues, published on Journal of Endodontics in 2012, documents healing rates of 94% for endodontic microsurgery performed under a microscope, compared to 88% without magnification. In absolute terms it seems like a modest difference. In clinical terms, that means one in six fewer patients requiring a second operation.
The most significant data concerns the MB2 canal — the second mesiobuccal canal of the upper molars. This channel escapes detection with the naked eye in 40-60% of cases. With the microscope, the identification rate exceeds 90% (Buhrley et al., Journal of Endodontics, 2002). An untreated canal is an infected canal: the most frequent cause of endodontic failure and post-treatment pain.
The consensus published on BMC Oral Health in 2023 indicates the operating microscope as the reference standard for conservative endodontics and apical microsurgery.
Beyond endodontics: where everything changes
The microscope is not an endodontic instrument. It is a precision instrument that crosses every discipline.
In prosthetics, the margin control at 20× guarantees a marginal closure that is impossible to verify with the naked eye. When working with feldspar ceramic veneers 0.3 mm thick, every hundredth of a millimeter of marginal gap is visible — and treatable — only under magnification. The result is a more precise adhesion and significantly greater longevity of the restoration.
In regenerative surgery, suturing under a microscope (microsurgery) uses 6-0 and 7-0 threads — thicknesses that the naked eye struggles to distinguish. Tissues heal with less inflammation, less tension, less risk of dehiscence. For the patients they face implant procedures with bone regeneration — including the maxillary sinus lift — the difference in the quality of healing is tangible.
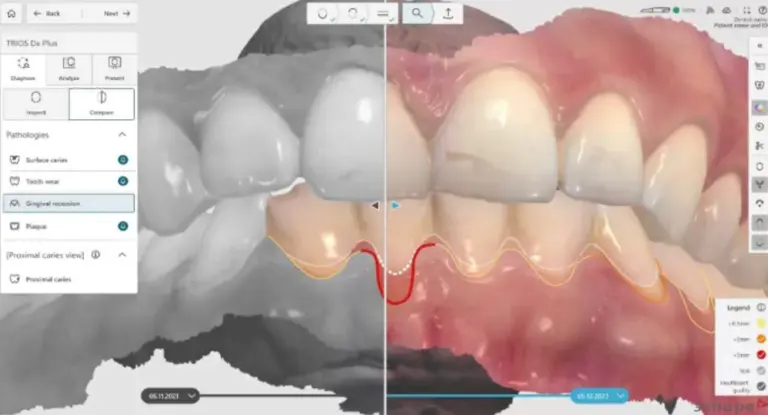
In diagnostics, the microscope is the first instrument of investigation — already from first dental visit — for vertical fractures, recurrent caries under existing restorations, and evaluation of suspect tissue. It sees earlier, it sees better, and allows intervention before the damage progresses.
A protocol, not an accessory
In many studies the microscope is present but used occasionally - for "difficult" cases, for extreme situations. In the Buniato Studio the microscope is integrated into the standard protocol of every root canal treatment, every microsurgery, every prosthetic precision check.
This choice is not random. The clinical experience gained in international reference centers - from Zurich to Vienna - has consolidated a conviction: magnification is not optional for complex cases. It is the baseline for each case. Because even seemingly simple cases can hide unexpected anatomies, and seeing them up front is the difference between a successful treatment and one that requires a second operation.
The Leica M525 is a surgical grade device, originally designed for neurosurgery and ophthalmic microsurgery. Bringing it into daily dental practice means applying the same standard of visual precision to the teeth as is used on the brain.
The microscope from the patient's point of view
For the patient, the difference is not abstract. It results in shorter sessions — because the clinician identifies the problem on the first try. Less post-operative pain — because less healthy tissue is removed. Fewer retractions — because no channel is forgotten. In prosthetic restorations that last longer — because the margins are checked at magnifications that guarantee precision.
And there is a less obvious aspect: documentation. Each procedure under the microscope is recorded in high-resolution video and photography. The patient can see exactly what was done, why, and what the end result looks like. Transparency is not a stated value — it is a natural outcome of technology.
For those looking for a dentist who combines technology and clinical rigor, the operating microscope is one of the most reliable indicators of the quality of a study.
Frequently Asked Questions about the Operating Microscope
Is a microscope necessary for all root canal treatments?
Every root canal treatment benefits from magnification: the identification of accessory canals (such as the MB2 of the upper molars) goes from 40-60% to over 90% under the microscope. In the Buniato practice, the Leica M525 is used as standard in every endodontic treatment, not just in complex cases.
Does the microscope treatment last longer?
No. The expanded view allows you to identify anatomical structures more quickly, reducing search times and repeated steps. Initial accuracy reduces the need for subsequent corrections.
Is the operating microscope the same as magnifying lenses (loupes)?
No. The loupes offer magnifications of 2-6× with non-coaxial front light. The Leica M525 operating microscope reaches 25× with integrated LED coaxial illumination, stable stereoscopic field and video documentation. The difference is qualitative: the microscope eliminates shadows, maintains depth of field and allows you to operate with a precision inaccessible to loupes.
How can I book a visit to Studio Buniato?
For an evaluation that integrates operative microscopy, 3D CBCT diagnostics and intraoral scanner, the secretariat of the Buniato Dental Practice in Corso Francia 30 in Turin can be reached at 011 4373857 or via book.alfadocs.com.
Sources
- Setzer FC, Shah SB, Kohli MR, Karabucak B, Kim S. “Outcome of endodontic surgery: a meta-analysis of the literature — Part 1: Comparison of traditional root-end surgery and endodontic microsurgery.” Journal of Endodontics, 2010;36(11):1757-1765. DOI: 10.1016/j.joen.2010.08.007
- Buhrley LJ, Barrows MJ, BeGole EA, Wenckus CS. “Effect of magnification on locating the MB2 canal in maxillary molars.” Journal of Endodontics, 2002;28(4):324-327. DOI: 10.1097/00004770-200204000-00016
- Del Fabbro M, Corbella S, Tsesis I, Zevin B, Tiossi R. “Microscope versus endoscope in root-end surgery: a systematic review and meta-analysis.” BMC Oral Health, 2023;23:195. DOI: 10.1186/s12903-023-02888-x