CBCT (Cone Beam Computed Tomography) is a three-dimensional radiological examination that allows the anatomical structures of the oral cavity to be visualized with a precision not achievable by traditional radiography, using doses of radiation that are contained and modulated based on the specific clinical question.
Those who are faced with implant surgery, a complex endodontic evaluation or jaw surgery often find themselves faced with a concrete question: is a 3D CT scan really necessary? And how much radiation does it involve?
These are legitimate questions. The answer requires distinguishing between what two-dimensional radiography can show and what only the third dimension makes visible, without underestimating the issue of dose.
What does CBCT see that a traditional x-ray doesn't show
A panoramic radiograph (OPG) provides a two-dimensional image in which the structures overlap. This is sufficient for many routine evaluations, but becomes a limitation when the clinician needs to accurately measure the bone volume available for an implant, locate a root fracture, or map the course of the inferior alveolar nerve prior to surgery.
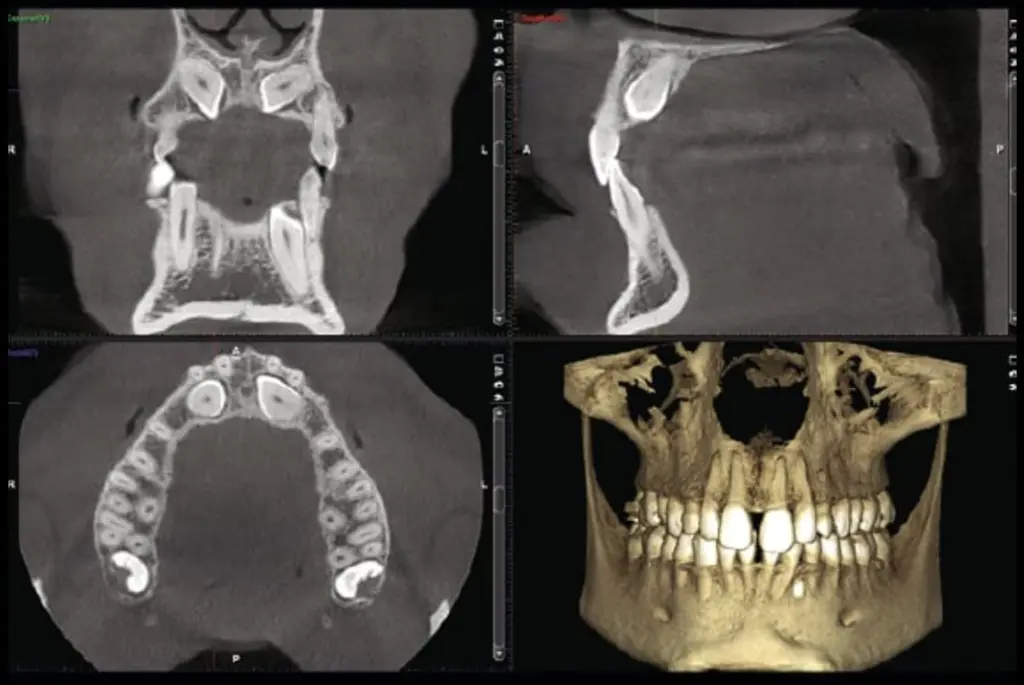
CBCT reconstructs a three-dimensional volume of the examined district: the dentist can navigate the anatomy layer by layer, measure real distances and not projections, and identify structures that would remain hidden in two dimensions. In our studio we use the system CBCT Planmeca, which allows you to select the field of view (FOV) and exposure parameters based on the specific clinical question.
When CBCT is clinically indicated
The test is prescribed when the expected diagnostic benefit exceeds the radiological risk and when the necessary information cannot be obtained with lower dose techniques. The main indications in dentistry include:
- Implantology: three-dimensional planning of implant insertion with exact knowledge of bone thickness and height, density of the recipient site and position of the noble structures. In our practice, CBCT is integrated into the Nobel Biocare implant workflow for guided design.
- Complex endodontics: root fractures, atypical root canal anatomy, complications of previous treatments. The literature confirms that CBCT maintains reliable diagnostic accuracy for the evaluation of endodontic conditions even with reduced dose protocols (Al-Haj Husain et al., 2026), supporting the work under operating microscope.
- Third molar surgery: when the overview suggests proximity between the roots of the wisdom tooth and the alveolar nerve canal, the CBCT clarifies the real spatial relationship.
- Periapical and periodontal pathology: lesions not evident on conventional radiography or complex bone defects requiring volumetric evaluation.
Not all situations require CBCT. An initial cavity, a routine check-up or a basic periodontal evaluation are managed with intraoral or panoramic radiography. The choice of exam always follows the clinical question.
The dose question: concrete data
The fear of radiation is understandable, but it deserves to be contextualized with the available data. A systematic review that analyzed 23 studies identified at least 13 modifiable technical factors that influence the effective dose of a CBCT: these include voltage (kV), amperage (mA), field of view (FOV), rotation angle, voxel size and exposure time (Moura et al., 2019).
This means that the dose is not a fixed value: it depends on how the exam is set up and what anatomical volume is acquired. Using a small FOV centered on the area of interest significantly reduces exposure compared to a full skull scan.
Research has also shown that it is possible to reduce the CBCT dose by approximately 20% compared to the manufacturer's standard parameters without compromising diagnostic accuracy for root fracture detection (Yalda et al., 2022). The same study highlighted that the high resolution setting does not significantly improve accuracy compared to standard parameters: a fact that reinforces the importance of choosing the appropriate protocol for the question, avoiding unnecessary exposures.
The systematic review also found that different CBCT scanners, with similar exposure parameters, produce significantly different effective doses (Moura et al., 2019). The choice of equipment is not a secondary detail.
How we use CBCT in our practice in Turin
In our practice in Corso Francia 30, Turin, the Planmeca CBCT is part of an integrated diagnostic flow. The test is prescribed when the clinical question justifies it and is performed with parameters optimized for the specific case, selecting field of view and resolution based on the necessary information.
The acquired three-dimensional data integrates with the scans of the 3Shape TRIOS 6 intraoral scanner and with direct clinical analysis to build a complete diagnostic picture. In implantology, this allows you to plan the position, inclination and depth of the implant before surgery. In endodontics, the three-dimensional map guides the work under the Leica operating microscope.
The goal is not to do more tests, but to do the right tests: those that concretely change the diagnosis and the treatment plan.
Frequently asked questions
Is CBCT painful or invasive?
No. The exam lasts a few seconds, requires no preparation and does not involve physical contact other than positioning the chin on the appropriate support. The patient remains standing or sitting and the device rotates around the head without touching it.
How much radiation does a CBCT involve compared to a traditional CT scan?
The dose of a dental CBCT is significantly lower than that of a conventional multislice CT of the facial massif. The actual dose depends on the parameters used and the selected field of view. As documented in the literature, at least 13 technical factors can be optimized to contain exposure while maintaining diagnostic quality (Moura et al., 2019).
Do all patients have to have CBCT?
No. CBCT is prescribed only when the clinical question cannot be resolved with conventional radiography. For routine checks, simple caries or standard periodontal evaluations, intraoral radiography or panoramic imaging remain the reference tests. The three-dimensional examination is reserved for cases in which the additional information concretely modifies the diagnosis or treatment plan.
Is CBCT safe in pregnancy?
As with any radiological examination, CBCT in pregnancy is evaluated on a case-by-case basis according to the principle of justification. In general, non-urgent radiological tests are postponed until after delivery. In case of documented clinical need, the clinician evaluates the risk-benefit ratio with the patient.
For a personalized evaluation of your case, Dr. Buniato is available for one first specialist visit with complete diagnostic analysis.
Sources
- Moura WS, Chiqueto K, Pithon GM, Neves LS, Castro R, Henriques JFC. Factors influencing the effective dose associated with CBCT: a systematic review. Clin Oral Investig. 2019;23(3). doi:10.1007/s00784-018-2561-4. Available on: PubMed.
- Yalda FA, Theodorakou C, Clarkson RJ, Davies J, Feinberg L, Sengupta A. Determination of a cone-beam CT low-dose protocol for root fracture diagnosis in non-endodontically treated anterior maxillary teeth. Dentomaxillofac Radiol. 2022;51(2):20210138. doi:10.1259/dmfr.20210138. Available on: PubMed.
- Al-Haj Husain A, Mergen V, Al-Haj Husain N, Alkadhi H, Demmert TT, Essig H. Photon-counting detector vs. cone-beam CT in endodontics: a study of simulated endodontic conditions, treatments, and associated complications. BMC Oral Health. 2026;26. doi:10.1186/s12903-026-07765-1. Available on: PubMed.