In summary. Full arch rehabilitation with All-on-4 or All-on-6 replaces all the teeth in an arch with a fixed prosthesis screwed onto four or six implants. The indication is established starting from the bone quality and volume measured with CBCT, not from the desire to have "fixed teeth the same day": immediate loading is only possible when the primary stability of the implants is adequate, and in some clinical conditions the protocol is not indicated at all.
What are All-on-4 and All-on-6
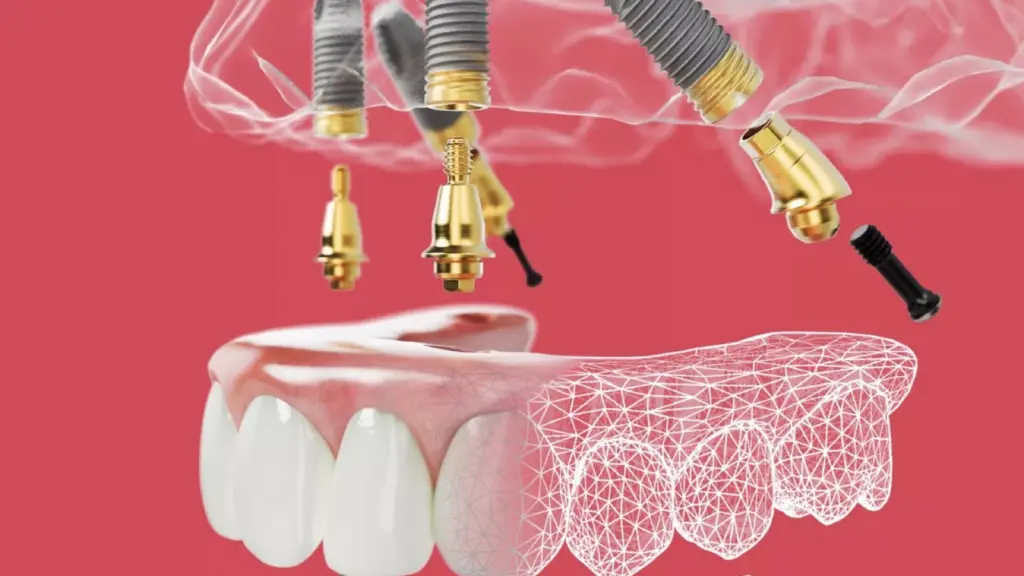
All-on-4 and All-on-6 are two variations of the same concept: an entire dental arch supported respectively by four or six implants, onto which a fixed prosthesis is screwed. They are designed for the person with a completely edentulous arch, or with non-recoverable residual teeth destined for extraction. Compared to the total removable prosthesis, the fixed solution provides stable chewing and does not rest on the mucosa. The technical characteristic of the All-on-4 approach is the inclination of the two posterior implants, which allows the available bone to be exploited, avoiding, in many cases, extensive grafts. It is not a solution "for everyone" and it is not a shortcut: it is a protocol with precise selection criteria, which start with diagnostics.
Who is the candidate: bone quality is measured, not assumed
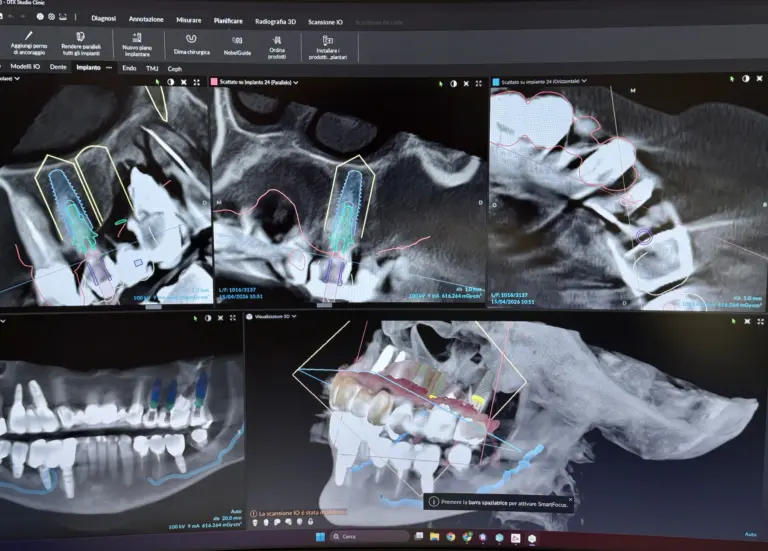
The candidate for fixed arch rehabilitation is the edentulous or close to edentulous person in whom the residual bone, due to volume and density, can guarantee the primary stability of the implants on the day of surgery. This evaluation is not done by eye or on orthopantomography alone: it requires a cone beam computed tomography (CBCT), which in the Buniato Study is acquired with the Planmeca VISO G3. The three-dimensional exam measures the height and thickness of the bone crest, identifies the structures to be respected (maxillary sinus, inferior alveolar nerve, foramina) and allows you to plan the position, length and inclination of each implant before entering the room. It is the phase that distinguishes a planned rehabilitation from an improvised one. Where the bone is sufficient and the density allows good initial anchorage, the case is favorable; where it is lacking, alternatives such as additional systems, regenerative techniques or deferred loading are evaluated. The general medical condition, smoking and oral hygiene are included in the same analysis: they are variables that weigh on the long-term prognosis.
All-on-4 or All-on-6: what's the real difference?
The difference is not "more implants, more safety", but a choice guided by the anatomy and the forces at play. All-on-6 distributes the load over a greater number of implants and can be preferred when the bone allows it and the occlusal framework requires it; All-on-4 reduces the number of implants and, with the inclination of the posterior ones, limits the use of grafts. From the point of view of documented results, a randomized clinical trial that directly compared the two configurations at five years found no statistically significant differences in implant survival or marginal bone loss between the two groups (Tallarico et al., 2016): both performed as predictable options in the medium term. This means that the decision between four and six implants is made on a case-by-case basis, on the basis of the CBCT and the prosthetic plan, and not on the basis of an alleged superiority of one of the two schemes. Anyone looking for a single answer that applies to everyone is asking the wrong question.
The computer-guided surgical-prosthetic protocol
Three-dimensional planning translates into guided surgery: on CBCT data, integrated with the optical scan of the arches acquired with the scanner 3Shape TRIOS 6, the position of each implant is designed and, when indicated, a surgical guide is created which transfers the project to the mouth. The digital flow reduces approximation: the implant position is decided in the study phase, not improvised during the operation, and is consistent with the prosthetic project from the beginning. The implants used are Nobel Biocare branded. During the operation, the primary stability of each implant is measured: this is the data that establishes whether it is possible to proceed with immediate loading or whether it is better to wait for osseointegration. Intra- and post-operative pain is controlled with local anesthesia and pharmacological management of the course; the declared objective is not a promise of absence of discomfort, but a predictable and monitored path.
Immediate load: when it is possible and what the literature says
Immediate loading - i.e. the application of a temporary fixed prosthesis in the hours following the operation - is not automatic: it depends on the primary stability achieved by the implants. When this is adequate, the literature does not highlight clinically relevant disadvantages compared to conventional deferred loading: a Cochrane systematic review on implant loading times found no convincing evidence of a clinically important difference in prosthetic failures, implant failures or bone loss between immediate loading and conventional loading (Esposito et al., 2013). In other words, immediacy is not a compromise on safety when conditions allow it; but it remains a conditioned possibility, not a right acquired through intervention. If stability is not sufficient, the correct choice is to postpone the load: forcing in these conditions increases the risk of failure.
The provisional same day and the final materials
When immediate loading is indicated, the fixed temporary prosthesis can be made the same day. The digital flow allows the temporary to be milled or printed on site: the practice uses chairside 3D printing with the SprintRay MIDAS system, which reduces waiting times and allows the delivery of a fixed screw-retained solution in the same operational phase. The provisional is not the finish line, but a stage: it accompanies healing and osseointegration for a few months, during which functional and aesthetic adaptation occurs. Only at the end of this phase is the definitive prosthesis created, with materials chosen according to the case - titanium or zirconia structures with aesthetic coating. The provisional-definitive sequence is not a duplication of work: it is the way in which the result is checked before making it stable.
Maintenance and controls over time
Fixed rehabilitation of the arch does not end with the delivery of the definitive prosthesis: maintenance begins there. Periodic clinical and radiographic checks and dedicated professional hygiene sessions are foreseen, because the screw-retained prosthesis requires specific cleaning of the underlying spaces. Long-term data support the choice when the path is followed consistently: a longitudinal study on mandibular All-on-4 with follow-up up to 18 years reports a prosthetic survival of 98.8% and an implant survival of 93% (Malò et al., 2019). However, the same data show that biological and mechanical complications can occur and that smoking and poor maintenance increase the probability: longevity does not depend on the intervention alone, but is built over time together with the patient.
When fixed arch rehabilitation is NOT indicated
There are situations in which the protocol is not the correct choice, and declaring this is part of the clinical evaluation. It is not indicated in the presence of non-stabilised periodontitis: active infection and inflammation must be treated and brought under control before any implant insertion, otherwise the prognosis is affected. It is not indicated when expectations are unrealistic, for example the request for a result without intermediate phases, without maintenance or without biological limits: serious rehabilitation is based on shared and verifiable objectives. And it is not indicated when the person is not in a position to guarantee the necessary follow-up and home and professional hygiene: without maintenance, the risk of complications increases and the advantage of the fixed solution is reduced. In these cases, alternatives are discussed, from preliminary periodontal stabilization to other prosthetic paths. The criterion is always the same: the real prognosis, not the technical feasibility of the intervention itself.
Frequently asked questions
Will I really have fixed teeth on the same day as the surgery?
Only if the primary stability of the implants measured during the operation is adequate. In that case, a fixed temporary prosthesis is applied, screwed on the same day, which can be made with 3D printing on site. If stability is not sufficient, the correct choice is to wait for osseointegration: forcing immediate loading in unfavorable conditions increases the risk of failure.
Better All-on-4 or All-on-6?
There is no one-size-fits-all answer. The choice depends on the bone volume and density detected with CBCT and the prosthetic design. A five-year randomized study found no statistically significant differences in survival or bone loss between the two configurations: both remained predictable medium-term options. The decision is made on a case-by-case basis.
Is the temporary also the definitive prosthesis?
No. The temporary accompanies the healing and osseointegration phase for a few months. The definitive prosthesis is created at the end of this phase, with materials chosen based on the case, such as titanium or zirconia structures with aesthetic coating.
How long does an All-on-4 rehabilitation last?
Long-term data are favorable when maintenance is constant: a study with follow-up up to 18 years reports a prosthetic survival of 98.8% and implant survival of 93%. The actual duration depends on hygiene, periodic checks and individual factors such as smoking, which increases the risk of complications.
I have periodontitis: can I still have this procedure?
Not as long as periodontitis is active. Infection and inflammation must be stabilized before inserting implants, because uncontrolled periodontitis worsens the prognosis. Periodontal stabilization is a preliminary stage, not a definitive obstacle.
Is a bone graft always necessary?
Not always. The inclination of the posterior implants in the All-on-4 approach allows in many cases to exploit the available bone while avoiding extensive grafts. The need for bone regeneration is established on the basis of CBCT, on a case-by-case basis.
Sources
- Soto-Penaloza D, Zaragozí-Alonso R, Peñarrocha-Diago M, Peñarrocha-Diago M. The all-on-four treatment concept: Systematic review. J Clin Exp Dent. 2017;9(3):e474-e488. doi:10.4317/jced.53613. PubMed.
- Malò P, de Araújo Nobre M, Lopes A, Ferro A, Botto J. The All-on-4 treatment concept for the rehabilitation of the completely edentulous mandible: A longitudinal study with 10 to 18 years of follow-up. Clin Implant Dent Relat Res. 2019;21(4):565-577. doi:10.1111/cid.12769. PubMed.
- Tallarico M, Meloni SM, Canullo L, Caneva M, Polizzi G. Five-Year Results of a Randomized Controlled Trial Comparing Patients Rehabilitated with Immediately Loaded Maxillary Cross-Arch Fixed Dental Prosthesis Supported by Four or Six Implants Placed Using Guided Surgery. Clin Implant Dent Relat Res. 2016;18(5):965-972. doi:10.1111/cid.12380. PubMed.
- Esposito M, Grusovin MG, Maghaireh H, Worthington HV. Interventions for replacing missing teeth: different times for loading dental implants. Cochrane Database Syst Rev. 2013;(3):CD003878. doi:10.1002/14651858.CD003878.pub5. PubMed.
For an evaluation of your specific case, the first specialist visit includes the complete diagnostic analysis, with the CBCT study necessary to establish the most suitable indication and configuration.